Peptic Ulcer Disease (PUD)
Definition of Peptic Ulcer Disease:
- Focal defects in the gastric mucosa that penetrate the muscularis mucosal layer results in scarring. In contrast, damage that remains above the muscularis mucosa is considered an erosion and typically heals without scarring.
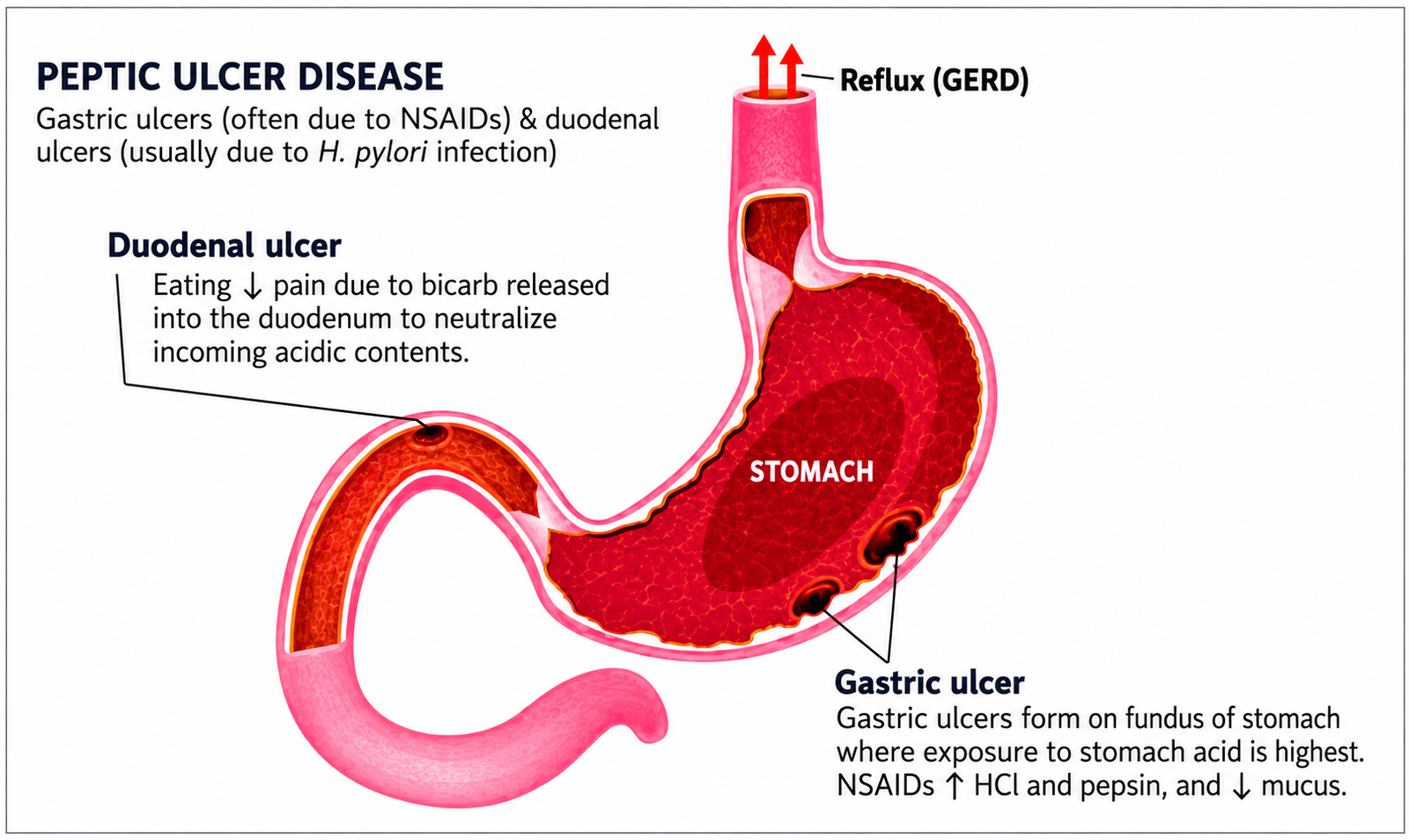
- Peptic ulcer disease includes defects in the stomach (gastric ulcers) and duodenum (duodenal ulcers)

Illustration of the different layers of the stomach wall.
Types of Peptic Ulcers
Peptic ulcers are mainly classified based on their location:
- Gastric ulcers – occur in the stomach
- Duodenal ulcers – occur in the upper part of the small intestine
These ulcers can be effectively diagnosed using upper gastrointestinal endoscopy
Common Causes of Peptic Ulcer Disease
The majority of peptic ulcers are caused by:
- Helicobacter pylori (H. pylori) infection – responsible for around 70–95% of cases
- Non-steroidal anti-inflammatory drugs (NSAIDs) – including aspirin
- Smoking & Stress-related ulcers – often seen in critically ill or mechanically ventilated patients
Less Common Causes
Other less frequent causes of PUD include:
- Hypersecretory conditions such as Zollinger-Ellison syndrome
- Viral infections (e.g., cytomegalovirus)
- Radiation therapy
Inflammatory conditions like Crohn’s disease
Helicobacter pylori: Structure, Virulence Factors and Role in Disease
Overview of Helicobacter pylori
Helicobacter pylori (H. pylori) is a gram-negative, spiral-shaped gram-negative bacterium that plays a major role in the development of peptic ulcer disease and chronic gastritis. It is specially adapted to survive in the acidic environment of the stomach.

Colorful educational illustration of Helicobacter pylori demonstrating urease activity, ammonia cloud formation, type IV secretion system, and major virulence factors involved in gastric disease.
Structure and Motility
H. pylori has multiple flagella at one end, which provide motility. This allows the bacterium to move through the stomach lining and penetrate beneath the protective mucus layer, where it attaches to the epithelial surface.
Adhesion Mechanism
The bacterium uses a specific adhesion protein known as BabA to bind to Lewis b antigens present on gastric epithelial cells. This attachment helps H. pylori colonise and persist within the stomach lining.
Survival in Acidic Environment
Although the stomach is highly acidic, H. pylori survives by producing the enzyme urease. This enzyme breaks down urea into ammonia, which neutralises the surrounding acid and creates a more favourable environment for the bacterium.
Colonisation Sites
H. pylori primarily colonises gastric-type epithelium. It is only found in the duodenum when there are areas of gastric metaplasia, where the tissue resembles that of the stomach.
Pathogenesis and Inflammatory Response
H. pylori causes chronic gastritis by triggering an inflammatory response in the gastric mucosa. The severity of disease depends on several bacterial factors, including specific virulence genes.
Key Virulence Factors
cagA Gene
Some strains of H. pylori produce the cagA protein, which is injected into host epithelial cells. This protein interferes with normal cell signalling pathways, affecting cell growth and programmed cell death (apoptosis). Strains that carry the cagA gene are more strongly associated with disease.
vacA Toxin
Most H. pylori strains produce a toxin called vacA. This toxin increases cell membrane permeability, causes loss of essential nutrients, promotes cell damage, and suppresses immune responses. Certain forms of vacA, particularly the s1/m1 type, are linked with more severe disease.
Pathophysiologyof Peptic Ulcer Disease: Balance Between Acid and Mucosal Defense
Under normal conditions, the gastrointestinal tract maintains a balance between acid production and protective mechanisms. These defense mechanisms include:
- Mucus and bicarbonate secretion
- Adequate mucosal blood flow
- Prostaglandin production
- Cellular repair and regeneration
These protective factors help shield the mucosa from harmful agents such as gastric acid, pepsin, NSAIDs, and H. pylori. When this balance is disrupted, mucosal damage occurs, leading to the development of peptic ulcers.
Clinical Features / Symptoms of Peptic Ulcer Disease
Peptic ulcer disease (PUD) is a chronic relapsing condition characterized by periods of exacerbation and remission that may continue for many years. The most common presenting symptom is dyspepsia, although only a small proportion of patients with dyspepsia are ultimately found to have an ulcer.
The hallmark symptom of PUD is epigastric pain or discomfort, often described as a gnawing, burning, aching, or hunger-like sensation located in the middle or upper abdomen, occasionally localizing to the tip of the xiphoid process. The pain typically shows a characteristic relationship to meals and often occurs in recurrent episodes separated by symptom-free periods.

How Duodenal Ulcers Develop – Step-by-Step Pathophysiology Diagram
Duodenal Ulcers
Duodenal ulcer pain classically:
- Develops 1–3 hours after meals, when the stomach is relatively empty.
- Is often worse at night and may awaken the patient from sleep.
- Is typically relieved by food, milk, or antacids.
- Tends to occur in clusters over several weeks, followed by periods of remission.
Gastric Ulcers
Symptoms of gastric ulcers are often less typical and less predictable than those of duodenal ulcers. Pain may occur shortly after meals and is frequently aggravated by eating, which can lead to reduced food intake and weight loss. Because gastric ulcers may mimic gastric malignancy, endoscopic biopsy is required to exclude cancer.
Associated Symptoms
Additional symptoms may include:
- Heartburn
- Belching
- Abdominal bloating
- Cramping
- Nausea
- Vomiting
- Loss of appetite (anorexia)
- Early satiety
Vomiting occurs in approximately 40% of patients. Persistent or daily vomiting suggests the possibility of gastric outlet obstruction.
Atypical and Silent Presentations
The clinical presentation may be less characteristic in elderly patients and in those taking non-steroidal anti-inflammatory drugs (NSAIDs). In such cases, pain may be mild or absent, presenting only as vague epigastric discomfort, nausea, anorexia, or early satiety.
Some ulcers remain completely silent until complications develop. These patients may present for the first time with iron deficiency anaemia due to chronic occult blood loss, acute upper gastrointestinal bleeding, or perforation.
Complications
Peptic ulcer disease may present initially with one of its complications, including:
- Upper gastrointestinal bleeding (approximately 10%), which may be severe if a major vessel such as the gastroduodenal artery is involved.
- Perforation (approximately 2%), most commonly occurring with anterior ulcers.
- Gastric outlet obstruction (approximately 2%) due to oedema, inflammation, or scarring.
- Penetration into adjacent organs (approximately 2%), particularly posterior ulcers, which may involve the pancreas and cause pancreatitis.
Although certain symptom patterns are classically associated with peptic ulcer disease, the diagnostic value of history alone is limited, and clinical symptoms cannot reliably distinguish peptic ulcer disease from functional dyspepsia. Definitive diagnosis therefore requires endoscopic evaluation when clinically indicated.
H. PYLORI DETECTION AND MANAGEMENT
| Test | Advantages | Disadvantages |
|---|---|---|
| Serology (non-invasive) | Rapid office kits availableGood for population studies | Lacks specificityCannot differentiate current from past infection |
| C-urea breath test | High sensitivity and specificity | Requires expensive mass spectrometer |
| Faecal antigen test | CheapSpecific (>95%) | Acceptability issues |
| Histology (invasive antral biopsy) | High specificity | False negativesTakes several days to process |
| Rapid urease test | Cheap, quick, specific (>95%) | Sensitivity ~85% |
| Microbiological culture | Gold standard Defines antibiotic sensitivity | Slow and laboriousLacks sensitivity |
H. PYLORI Diagnostic Tests
Common, non-invasive, diagnostic tests for H. pylori include the urea breath test (UBT), which detects gas CO2 produced by the bacteria, and the fecal antigen test, which detects H. pylori in the stool. PPIs, bismuth and antibiotics should be discontinued two weeks prior to these tests to avoid false negative results. The infection should be treated if testing is positive.
Best Treatment for Peptic Ulcer Disease (2026): Drugs & Guidelines
Non-Pharmacological Treatment of Peptic Ulcer Disease- 2026
In addition to medications, lifestyle and dietary modifications play an important role in the management of peptic ulcer disease. These non-pharmacological measures can help reduce symptoms, promote healing, and prevent recurrence.
1. Dietary Modifications
A strict “bland diet” is no lon
ger routinely recommended. Instead, patients should follow a balanced diet with moderation and avoid foods that worsen symptoms.
Common food to avoid :
- Coffee and caffeinated beverages
- Spicy foods
- Fatty or fried foods
- Large or heavy meals
Tip: Patients are advised to identify and limit foods that personally trigger dyspepsia.
2. Smoking Cessation
Smoking has been shown to:
- Delay ulcer healing
- Increase gastric acid secretion
- Raise the risk of ulcer recurrence
Therefore, quitting smoking is strongly recommended, especially in patients with non–H. pylori ulcers.
Key Takeaway
Non-pharmacological strategies, including dietary control and smoking cessation, are essential components of peptic ulcer management and should be combined with appropriate medical therapy for optimal outcomes.
Management of Peptic Ulcer Disease algorithm

Clinical algorithm for diagnosis and management of suspected peptic ulcer disease.
Management of Peptic Ulcer Disease Based on Etiology | H. pylori, NSAID & Stress Ulcers Explained
Specific management of peptic ulcer disease depends on etiology
1. Management of H. pylori-associated Peptic Ulcer Disease: Eradication Therapy:

Stepwise algorithm for peptic ulcer disease (PUD) management covering alarm features, H. pylori testing, PPI therapy, and eradication strategies.
Drugs used in H. pylori eradication therapy 
Stepwise first-line treatment options for Helicobacter pylori infection showing standard eradication regimens used in clinical practice.
What are the first-line H. pylori eradication therapy regimens?
First-line H. pylori eradication therapy regimens typically include bismuth-based quadruple therapy, which is recommended by the American College of Gastroenterology due to increasing clarithromycin resistance and higher failure rates with triple therapy. Standard treatment combines a proton pump inhibitor (PPI) with two or more antibiotics, and sometimes bismuth, for 10–14 days to achieve effective bacterial eradication.
PPI-based triple therapy (PPI + clarithromycin + amoxicillin or metronidazole) is only recommended in areas with low clarithromycin resistance (<15%) and in patients with no prior macrolide exposure. Drug substitutions are not recommended because they reduce eradication success rates, and PPIs should not be replaced with H2 blockers unless absolutely necessary.
Overall, guideline-directed therapy significantly improves eradication rates and reduces the risk of complications such as peptic ulcer disease and gastric cancer.
It is important that clinicians do not substitute drugs within regimens, as treatment efficacy may significantly decrease—H2 receptor antagonists should not replace PPIs unless intolerance occurs, and antibiotics should not be interchanged across classes (e.g., ampicillin should not replace amoxicillin). Proton pump inhibitors may be continued beyond 14 days only when needed for ulcer healing, but they are not intended for long-term use in eradication therapy. Proper adherence to guideline-based therapy significantly improves eradication success and reduces recurrence risk.

What are the alternative treatment options for H. pylori infection?
Alternative treatment options for H. pylori include sequential therapy, hybrid therapy, quinolone-based regimens, rifabutin-based therapy, and vonoprazan-based combination therapy. These regimens may be considered when first-line treatment is unsuitable, has failed, or when antibiotic resistance influences treatment selection.
What is sequential therapy for H. pylori eradication?
Sequential therapy is a two-phase treatment regimen for H. pylori. Patients typically receive a proton pump inhibitor (PPI) plus amoxicillin for the first 5–7 days, followed by a PPI combined with clarithromycin and metronidazole for another 5–7 days. Although included in some treatment guidelines, sequential therapy generally has weaker supporting evidence than recommended first-line regimens.
What is hybrid therapy for Helicobacter pylori infection?
Hybrid therapy begins with a proton pump inhibitor (PPI) and amoxicillin for seven days. During the second week, clarithromycin and metronidazole are added while continuing the PPI and amoxicillin. This approach combines features of sequential and concomitant therapy but is supported by less clinical evidence than standard first-line treatments.
Are quinolone-based regimens recommended for H. pylori?
Quinolone-based regimens may be used in selected patients, particularly after treatment failure or when other antibiotics are unsuitable. However, current clinical guidelines generally consider these regimens to have weaker supporting evidence compared with first-line therapies such as bismuth quadruple therapy.
What is Talicia for H. pylori treatment?
Talicia is an FDA-approved combination medication used to treat H. pylori infection. Each capsule contains rifabutin, amoxicillin, and omeprazole, providing antibiotic therapy together with acid suppression to improve bacterial eradication.
What medications are included in Talicia?
Talicia contains three active ingredients:
- Rifabutin
- Amoxicillin
- Omeprazole
These medications work together to eliminate H. pylori bacteria while reducing stomach acid to improve treatment effectiveness.
What is vonoprazan and how does it treat H. pylori?
Vonoprazan is a potassium-competitive acid blocker (PCAB) that suppresses stomach acid. Unlike proton pump inhibitors (PPIs), it blocks acid secretion through a different mechanism and is used in several FDA-approved H. pylori treatment regimens.
What are Voquezna Dual Pak and Voquezna Triple Pak?
Voquezna Dual Pak contains:
- Vonoprazan
- Amoxicillin
Voquezna Triple Pak contains:
- Vonoprazan
- Amoxicillin
- Clarithromycin
These combination therapies use vonoprazan instead of a proton pump inhibitor to help eradicate H. pylori.
Is vonoprazan better than proton pump inhibitors for H. pylori treatment?
Vonoprazan provides rapid and potent acid suppression and is approved for use in specific H. pylori treatment regimens. However, the best treatment depends on antibiotic resistance, previous antibiotic exposure, allergies, local guidelines, and individual patient factors. Clinical recommendations continue to evolve as more evidence becomes available.
When are alternative H. pylori treatment regimens used?
Alternative treatment regimens are generally considered when:
- Standard first-line therapy has failed.
- Antibiotic resistance is suspected.
- The patient has medication allergies or intolerances.
- Previous antibiotic exposure limits treatment options.
- A clinician recommends a tailored regimen based on current guidelines.
NSAID-Induced Ulcers: Causes, Risk Factors, Prevention & Treatment
What Are NSAID-Induced Ulcers?
Non-steroidal anti-inflammatory drugs (NSAIDs), including commonly used medications like aspirin and ibuprofen, are a major cause of gastric (stomach) ulcers. These drugs damage the stomach lining through two key mechanisms:
- Direct irritation of the gastric epithelium
- Systemic inhibition of prostaglandin synthesis via COX-1 blockade
Prostaglandins normally protect the stomach lining by promoting mucus and bicarbonate secretion. When NSAIDs block this pathway, the stomach becomes vulnerable to acid injury, increasing the risk of ulcers and gastrointestinal (GI) bleeding.
Risk Factors for NSAID-Induced Gastric Ulcers
Certain patients are at significantly higher risk of developing NSAID-related ulcers. Key risk factors include:
- Age over 60 years
- History of peptic ulcer disease (PUD), including H. pylori-associated ulcers
- Use of high-dose NSAIDs
- Use of multiple NSAIDs (e.g., ibuprofen + aspirin)
- Concomitant use of:
- Anticoagulants
- Corticosteroids
- SSRIs or SNRIs
Patients with multiple risk factors have a substantially increased risk of ulcer formation and GI bleeding.
NSAIDs, Cardiovascular and Renal Risk
All NSAIDs can:
- Increase blood pressure
- Reduce renal blood flow
- Worsen kidney function
Therefore, NSAIDs should be used cautiously in patients with cardiovascular disease (CVD) or renal impairment.
COX-2 Selective vs Non-Selective NSAIDs
NSAIDs differ in their COX enzyme selectivity:
COX-2 Selective NSAIDs
- Example: Celecoxib
- Lower GI ulcer risk
- Higher cardiovascular risk
Partially COX-2 Selective NSAIDs
- Meloxicam
- Nabumetone
- Diclofenac
- Etodolac
These drugs have intermediate GI and CV risk profiles.
Prevention of NSAID-Induced Ulcers
For patients at high GI risk, ulcer prevention is essential.
1. Proton Pump Inhibitors (PPIs)
- Reduce gastric acid secretion
- Lower risk of ulcer formation and GI bleeding
- Commonly used in long-term NSAID users
2. Misoprostol (Cytoprotective Agent)
- Prostaglandin E1 analogue
- Replaces protective prostaglandins depleted by NSAIDs
- Effective but limited by side effects (especially diarrhea)
3. Combination Formulations
To improve adherence and reduce ulcer risk:
- Naproxen + esomeprazole (Vimovo)
- Ibuprofen + famotidine (Duexis)
- Diclofenac + misoprostol (Arthrotec)
- Aspirin + omeprazole (Yosprala) – used for cardiovascular secondary prevention
NSAID Choice in High-Risk Patients
- High GI + high CV risk: Avoid NSAIDs if possible
- High CV risk + low GI risk: Naproxen is preferred
- Low CV risk: COX-2 inhibitors ± PPI may be used
Treatment of NSAID-Induced Ulcers
If an ulcer develops:
- Stop NSAIDs if possible
- Treat with a PPI for 8 weeks
- If PPIs cannot be used:
- High-dose H2 receptor antagonists
- Sucralfate
Cytoprotective Drugs Explained
Misoprostol
- Mechanism: prostaglandin replacement
- Dose: 200 mcg four times daily with food
- Side effects: diarrhea, abdominal cramps
- Important warning: contraindicated in pregnancy (abortifacient effect)
Sucralfate
- Forms a protective barrier over ulcers
- Dose: 1 g four times daily on an empty stomach
- Side effects: constipation
- Use caution in renal impairment (aluminium accumulation risk)
- Must be separated from other medications due to binding interactions
Key Clinical Takeaway
NSAID-induced ulcers are preventable. Proper risk assessment, rational NSAID selection, and prophylactic use of PPIs or cytoprotective agents significantly reduce complications such as gastrointestinal bleeding and perforation.

Leave a Reply