Gastro-oesophageal reflux disease (GORD/ GERD)
Gastric Acid Secretion, Proton Pump Mechanism, and GERD Explained

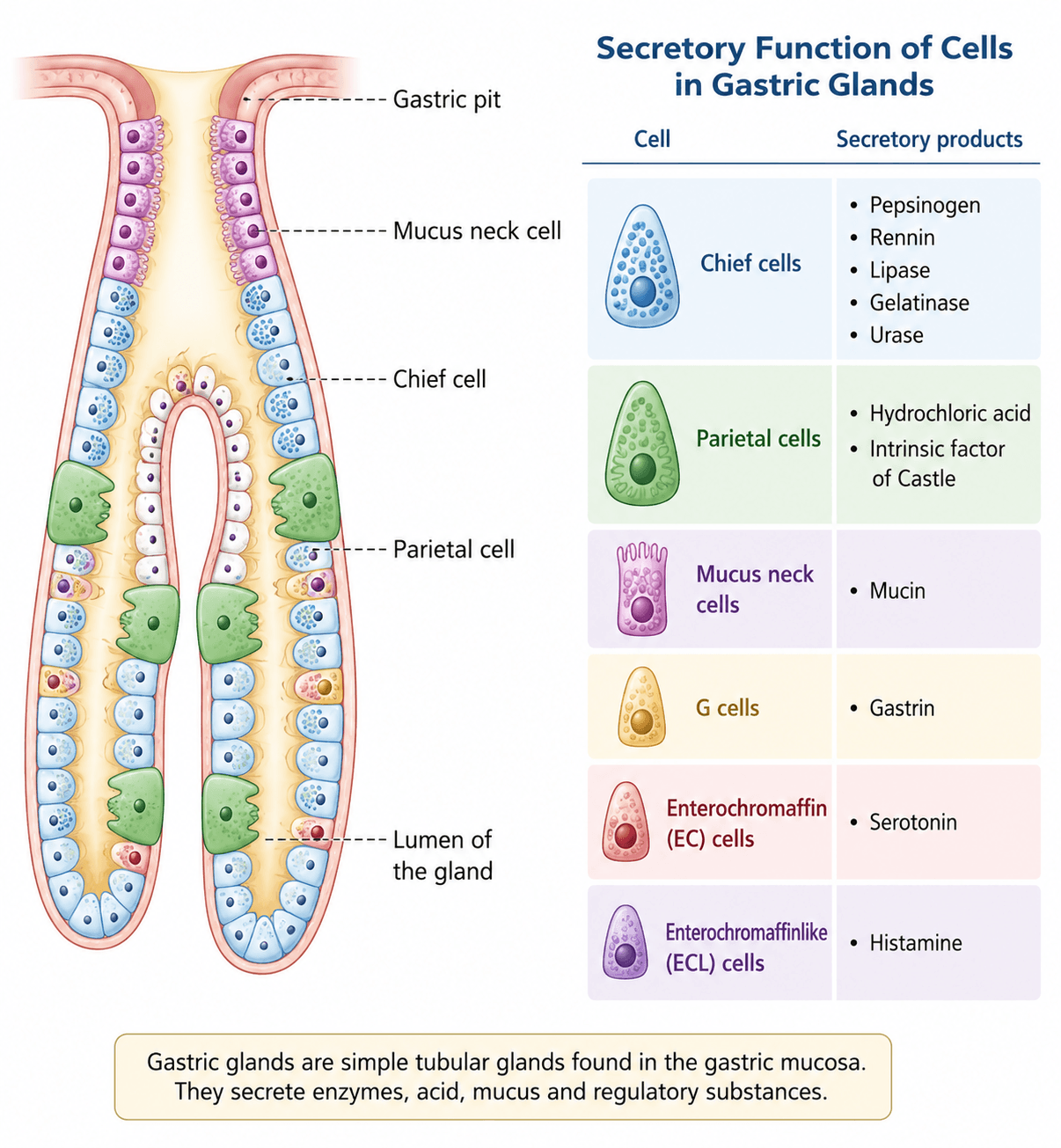
The human stomach plays a central role in digestion by producing hydrochloric acid (HCl), which helps break down food, activate digestive enzymes, and eliminate harmful microorganisms. This acid secretion is tightly regulated by specialized cells and hormonal signals to maintain digestive efficiency and protect the gastrointestinal tract.
How Stomach Acid is Produced
Parietal cells located in the epithelial lining of the stomach are responsible for secreting hydrochloric acid (HCl). This process occurs through the hydrogen-potassium adenosine triphosphatase (H⁺/K⁺-ATPase) pump, commonly known as the proton pump. This pump actively transports hydrogen ions (H⁺) into the stomach lumen in exchange for potassium ions (K⁺), leading to the formation of gastric acid.


The secretion of HCl is regulated by three key stimulators:
- Histamine
- Acetylcholine
- Gastrin
Among these, gastrin also plays an important role in stimulating gastric smooth muscle contractions, which enhances the mixing and movement of food during digestion.
Role of the Lower Esophageal Sphincter (LES)
Under normal physiological conditions, the acidic contents of the stomach are prevented from flowing back into the esophagus by a muscular valve known as the lower esophageal sphincter (LES). This sphincter maintains a one-way barrier between the stomach and esophagus, protecting the esophageal lining from acid damage.

Pathophysiology of GERD?
In patients with gastroesophageal reflux disease (GERD), the tone of the LES is reduced. This weakening allows gastric contents, including acid, to reflux or flow backward into the esophagus. This backflow can lead to symptoms such as heartburn, chest discomfort, and inflammation of the esophageal lining.

1. Obesity / Dietary factors
These increase pressure in the abdomen or trigger acid production.
Examples:
- Overeating large meals (e.g., buffet meals, heavy dinners)
- High-fat foods (fried chicken, burgers, pizza)
- Chocolate (relaxes the lower oesophageal sphincter)
- Caffeine (coffee, energy drinks)
- Alcohol (beer, wine, spirits)
- Spicy foods (chilli-based dishes)
- Late-night eating before bed
2. Defective oesophageal clearance
The oesophagus fails to push acid back into the stomach efficiently.
Examples:
- Weak peristalsis (common in older adults)
- Conditions like scleroderma
- Reduced saliva (dry mouth → less neutralization)
- Lying down immediately after eating
3. Abnormal lower oesophageal sphincter (LES)
The LES doesn’t close properly, allowing acid to reflux.
Examples:
- Naturally weak LES tone
- Temporary LES relaxation after meals
- Smoking (nicotine relaxes LES)
- Certain medications:
- Calcium channel blockers
- Nitrates
- Anticholinergics
4. Hiatus hernia
Part of the stomach moves up into the chest, weakening the LES barrier.
Examples:
- Sliding hiatus hernia (most common type)
- Seen more in:
- Older adults
- Obese individuals
- People with chronic coughing or straining
5. Delayed gastric emptying
Food stays longer in the stomach → more acid → higher reflux risk.
Examples:
- Gastroparesis (common in diabetes)
- Heavy fatty meals (slow digestion)
- Certain medications (opioids, antidepressants)
6. Increased intra-abdominal pressure
Pushes stomach contents upward into the oesophagus.
Examples:
- Pregnancy
- Obesity (especially central fat)
- Tight clothing (tight belts, jeans)
- Heavy lifting or straining
- Chronic constipation
7. Acid–pepsin (and bile) reflux
The damaging substances that irritate the oesophagus.
Examples:
- Stomach acid (HCl)
- Pepsin (protein-digesting enzyme)
- Bile reflux (in some cases, especially after surgery)

| Feature | Trivial to Mild GERD | Severe GERD |
|---|---|---|
| Frequency | < 3 times/week | Frequent (> 3/week) |
| Duration | Short | > 6 months |
| Intensity | Low | High |
| Pain score | 1–3 / 10 | 7–10 / 10 |
| Nocturnal symptoms | Absent | Present (awakens patient) |
| Effect on daily activity | No interference | Regular interference |
| Medical attention | Not required | Patient seeks physician |
| Complications | None | Present (due to acid reflux) |

DRUG TREATMENT
Antacids are commonly used medications that provide rapid relief from acid-related symptoms by neutralizing gastric acid, resulting in the formation of salt and water and an increase in gastric pH. Because antacids do not require systemic absorption, they act quickly—typically within minutes.
However, the duration of symptom relief is relatively short, usually lasting between 30 to 60 minutes, making them more suitable for mild and occasional symptoms of acid reflux or indigestion.
Antacids are widely available as over-the-counter (OTC) medications. Patients using antacids that contain aspirin (such as effervescent formulations) should be advised of the potential risk of gastrointestinal bleeding, especially with frequent or excessive use.
| DRUG | DOSING | SAFETY / SIDE EFFECTS / MONITORING |
|---|---|---|
| Calcium carbonate (Tums, others) + magnesium (Mylanta Supreme, others) + simethicone (anti-gas) (Maalox Advanced Maximum Strength, others) | Many formulations including suspensions, chewable tablets, capsules. Dosing varies by product; many require administration 4–6 times per day | WARNINGS Aluminum and magnesium: can accumulate with severe renal dysfunction (not recommended if CrCl < 30 mL/min); risk of bleeding with aspirin-containing products SIDE EFFECTS Unpleasant taste Calcium: constipation, bloating, belching Aluminum: constipation, hypophosphatemia Magnesium: loose stools (use with aluminum may counter-balance) NOTES Calcium-containing antacids may be preferred in pregnancy. Alka-Seltzer contains > 500 mg Na per tablet which can worsen edema in patients with heart failure or cirrhosis |
| Magnesium hydroxide (Milk of Magnesia, others) + aluminum (Mag-Al, others) + aluminum + simethicone (Mylanta Maximum Strength, others) | Many formulations including suspensions, chewable tablets, capsules. Dosing varies by product; many require administration 4–6 times per day | WARNINGS Aluminum and magnesium: can accumulate with severe renal dysfunction (not recommended if CrCl < 30 mL/min); risk of bleeding with aspirin-containing products SIDE EFFECTS Unpleasant taste Aluminum: constipation, hypophosphatemia Magnesium: loose stools (use with aluminum may counter-balance) |

Proton Pump Inhibitors (PPIs) – Simple Guide
What are PPIs?
Proton Pump Inhibitors (PPIs) are medicines that strongly reduce stomach acid by blocking the H⁺/K⁺ ATPase (proton pump) in stomach cells.
They are the most effective drugs for acid-related conditions like GERD.
How PPIs Work (Easy Memory Trick)
“PPI = Power Pump Inhibitor”
- Blocks final step of acid production

- Stops acid at the source
- Heals stomach & esophagus lining

When are PPIs used?
PPIs are commonly used for:
- GERD (acid reflux)
- Stomach ulcers
- Esophagitis (erosion of food pipe)
- Zollinger-Ellison syndrome (high acid condition)

Recommended timing for taking oral proton pump inhibitors (PPIs). This colorful infographic explains when to take esomeprazole, omeprazole, lansoprazole, pantoprazole, dexlansoprazole, and rabeprazole in relation to meals for optimal acid suppression and GERD treatment.

Comprehensive Proton Pump Inhibitor (PPI) products chart comparing dosing recommendations, safety warnings, common side effects, monitoring requirements, and clinical notes for commonly prescribed PPIs used to treat GERD, acid reflux, peptic ulcers, and other acid-related gastrointestinal disorders.
Risks Associated with Proton Pump Inhibitor (PPI) Therapy
Long-term proton pump inhibitor (PPI) therapy is highly effective for treating GERD, acid reflux, peptic ulcer disease, and other acid-related disorders, but prolonged use may increase the risk of certain health complications. By reducing stomach acid production, PPIs can cause chronic changes in gastric pH, creating an environment that may promote the growth of harmful microorganisms.
One of the primary concerns with long-term PPI use is an increased risk of gastrointestinal infections, particularly Clostridioides difficile (C. difficile) infection. Some studies also suggest a possible association between prolonged PPI therapy and community-acquired pneumonia, potentially due to the reflux and aspiration of gastric contents.
Extended use of PPIs has also been linked to a higher risk of osteoporosis-related bone fractures, especially in older adults and individuals receiving high-dose or long-duration treatment. For this reason, healthcare providers should periodically evaluate the need for continued therapy and use the lowest effective dose for the shortest appropriate duration whenever possible.
According to the Beers Criteria, proton pump inhibitors should generally not be used for longer than eight weeks in older adults unless there is a clear clinical indication. Appropriate long-term use may include patients at high risk of gastrointestinal bleeding, those requiring chronic NSAID therapy, or individuals who need maintenance treatment for specific gastrointestinal conditions.
Regular clinical review and individualized treatment decisions can help maximize the benefits of PPI therapy while minimizing potential long-term risks.
Drug Interactions and Precautions for Antacids, H2RAs, and PPIs
Antacids: Drug Interaction Precautions
Antacids can reduce the absorption of many medications by binding to them in the gastrointestinal tract. To minimize drug interactions, take antacids 2–4 hours before or 2–6 hours after other medications, depending on the specific drug. Always review potential interactions before combining antacids with prescription medicines.
H2 Receptor Antagonists (H2RAs): Safety and Drug Interactions
H2 receptor antagonists (H2RAs), such as famotidine and cimetidine, require caution in certain patient populations and when used with interacting medications.
- Use cautiously with central nervous system (CNS) depressants, especially in older adults, due to an increased risk of delirium, dementia, and cognitive impairment.
- Reduce the dose in patients with renal impairment.
- Avoid famotidine in patients taking medications with a high risk of QT interval prolongation.
- Cimetidine strongly inhibits CYP450 enzymes (CYP2C19, CYP3A4, CYP1A2) and may increase the effects of medications such as warfarin, phenytoin, clopidogrel, SSRIs, theophylline, amiodarone, and calcium channel blockers. Avoid combining cimetidine with dofetilide.
Proton Pump Inhibitors (PPIs): Important Drug Interactions
Proton pump inhibitors (PPIs) can interact with several commonly prescribed medications through CYP2C19 enzyme inhibition.
- All PPIs inhibit CYP2C19, with omeprazole and esomeprazole acting as moderate inhibitors.
- PPIs may increase blood levels of citalopram, phenytoin, tacrolimus, voriconazole, and warfarin.
- Avoid using PPIs with nelfinavir because they can reduce its effectiveness.
- Omeprazole and esomeprazole decrease the activation and effectiveness of clopidogrel, increasing the risk of cardiovascular events. These medications should not be used together.
- PPIs can reduce the renal elimination of methotrexate, increasing serum concentrations and the risk of methotrexate toxicity.
Leave a Reply