Crohn’s Disease: Symptoms, Causes, Diagnosis and Treatment (Complete 2026 Guide)
What Is Crohn’s Disease?
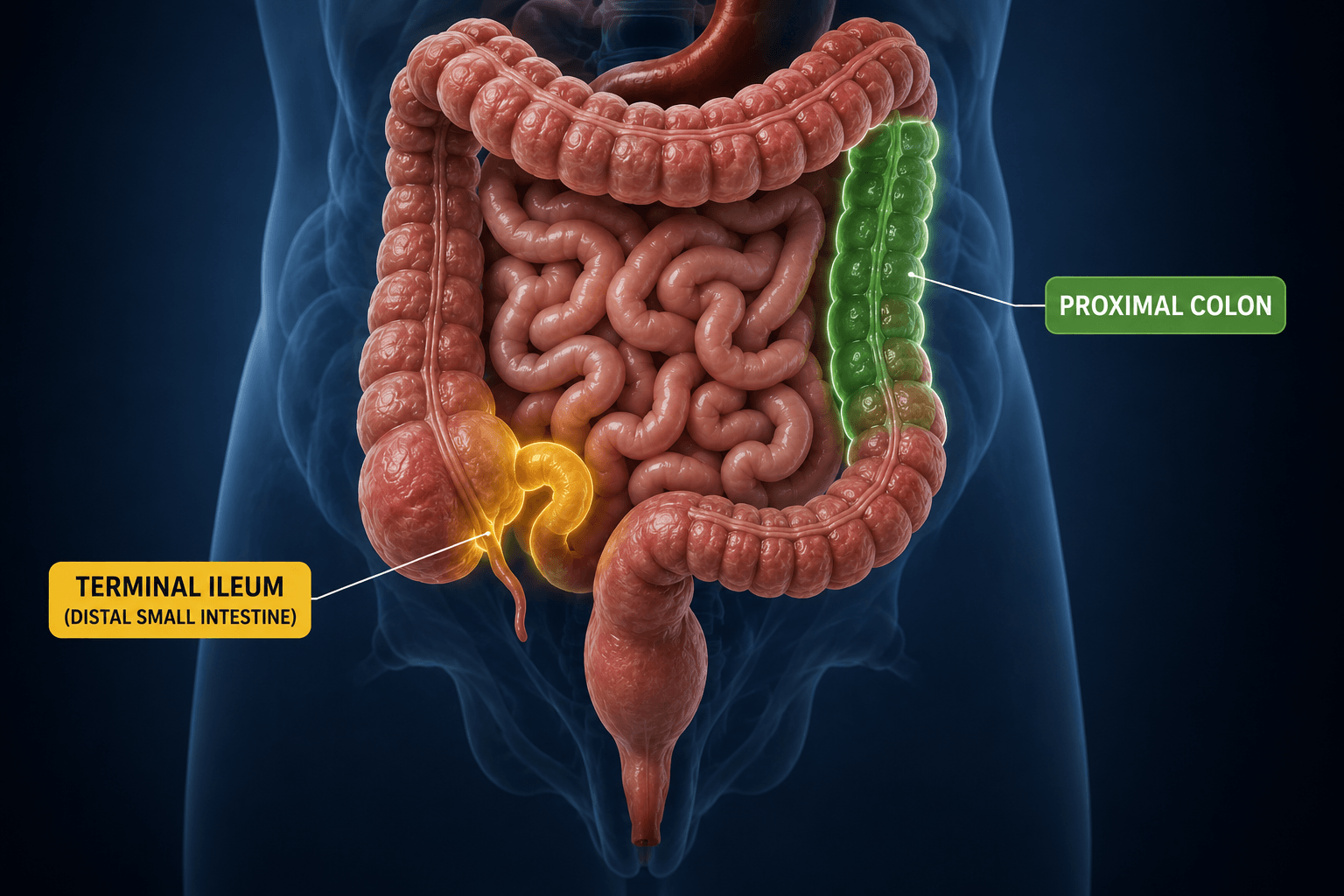
Crohn’s Disease is a chronic inflammatory disorder characterized by deep, transmural inflammation of the gastrointestinal tract. It can affect any part of the digestive system from the mouth to the anus, but it most commonly involves the terminal ileum (distal small intestine) and the proximal colon.

Highlighted regions show the terminal ileum and proximal colon, the most commonly affected areas in Crohn’s disease
ETIOLOGY AND PATHOGENESIS – For detailed explination click Here
Crohn’s Disease: Location of inflammation / Patterns of Disease Distribution
Crohn’s disease can present in several distinct anatomical patterns within the gastrointestinal tract. Understanding the distribution is important for diagnosis, clinical assessment, and treatment planning.
1. Ileum and Cecum Involvement (≈40%)
The most common pattern involves both the terminal ileum and the cecum, seen in around 40% of patients. This is also known as ileocecal Crohn’s disease and is a classic presentation.
2. Isolated Small Intestinal Disease (≈30%)
Approximately 30% of patients have disease confined to the small intestine, particularly the ileum. This form often leads to malabsorption, weight loss, and nutritional deficiencies.
3. Colonic Crohn’s Disease (≈25%)
In about 25% of cases, inflammation is limited to the colon only. This pattern may closely resemble ulcerative colitis clinically but differs in its transmural and patchy nature.
4. Upper Gastrointestinal Involvement (Rare)
Less commonly, Crohn’s disease can affect the upper gastrointestinal tract, including the mouth, tongue, esophagus, stomach, and duodenum. These presentations are uncommon but clinically significant when present.

Illustration showing the types of Inflammatory Bowel Disease (IBD), including Crohn’s disease and ulcerative colitis, with anatomical distribution and disease patterns in the gastrointestinal tract.
The inflammation can damage the intestinal wall and lead to complications such as intestinal strictures (narrowing of the bowel) and fistulas (abnormal connections between bowel loops or other organs).
Crohn’s Disease: Clinical Features, Symptoms, and Diagnostic Findings
Common Symptoms of Crohn’s Disease
Patients typically present with:
- Chronic diarrhea (often worse at night)
- Abdominal pain
- Unintentional weight loss
Diarrhea in Crohn’s Disease
Diarrhea is present in almost all patients with Crohn’s disease, but its characteristics depend on the site of intestinal involvement:
- Colonic disease (especially rectal involvement):
Diarrhea is usually small in volume and associated with urgency and tenesmus. Rectal inflammation reduces distensibility, so even small amounts of stool trigger a strong and urgent need to defecate. In chronic cases, scarring may lead to a rigid rectum and, in severe situations, fecal incontinence. - Small intestinal disease:
Stools are typically larger in volume and are not associated with urgency or tenesmus. - Terminal ileum involvement or post-surgical resection:
Patients may develop bile salt diarrhea or steatorrhea due to impaired bile salt absorption.
Abdominal Pain and Associated Symptoms of Crohn’s disease
The pattern of abdominal pain is closely related to disease location:
- In ileal Crohn’s disease, patients often experience cramping right lower quadrant pain, especially after meals. This is commonly due to partial, intermittent obstruction caused by a narrowed intestinal lumen.
- Associated symptoms may include abdominal distension, nausea, and vomiting.
Weight Loss and Systemic Features
Weight loss is common in most patients, regardless of disease location. It may result from malabsorption, reduced oral intake due to pain, diarrhea, or loss of appetite.
In some cases, perianal symptoms may appear early, sometimes even before intestinal symptoms develop. These include:
- Rectal bleeding
- Anal fissures (tears)
- Fistula formation
In many patients, the onset is gradual, and symptoms such as intermittent diarrhea and vague abdominal pain may persist for months or even years before a diagnosis is established.
Other systemic features include:
- Fever and chills during active disease
- Low-grade fever, which may be an early sign of a flare
- Improved energy and well-being following remission induced by treatment or surgery
Crohn’s disease follows a relapsing and remitting course, with periods of flare-ups and remission. In mild to moderate disease, spontaneous remission may occur in a proportion of patients, while relapse is also common over time.
Physical Examination Findings of Crohn’s disease,
Physical findings vary depending on disease severity and location:
- Oral lesions: Aphthous ulcers may be seen on the lips, gingiva, or buccal mucosa
- Abdominal tenderness: Usually localized to the area of active disease
- Palpable mass: Thickened bowel loops, mesentery, or abscess formation may produce a mass, commonly in the right lower quadrant
- Perianal disease: May present with fistulas, induration, redness, or tenderness around the anus
Laboratory Findings
Laboratory results are generally non-specific, although anemia is a common finding and may be related to chronic inflammation, blood loss, or nutritional deficiencies.
How Inflammatory Bowel Disease (IBD) is Diagnosed: Tests, Colonoscopy & Imaging Explained
Diagnosing inflammatory bowel disease (IBD) can be challenging because its symptoms often overlap with other common gastrointestinal conditions such as infections, constipation, diarrhoea, eating disorders, and peptic ulcer disease. Therefore, these alternative causes must be excluded before confirming a diagnosis.
Initial evaluation typically includes blood tests to detect markers of inflammation, such as C-reactive protein (CRP), along with stool tests like faecal calprotectin, which help identify intestinal inflammation. While these tests provide useful clues, they are not sufficient on their own.
The most definitive diagnostic procedure is a colonoscopy with biopsy, which allows direct visualisation of the colon and enables tissue sampling for histological analysis. In some cases, a sigmoidoscopy may be used, particularly when assessing suspected ulcerative colitis, as it examines the lower part of the bowel near the rectum.
If symptoms suggest involvement of the upper gastrointestinal tract, an upper endoscopy may be performed. Additionally, imaging techniques such as CT scans or MRI can help evaluate the extent of disease, detect complications, and support the overall diagnosis.
Endoscopic Differences Between Ulcerative Colitis and Crohn’s Disease
| Endoscopic Feature | Ulcerative Colitis (UC) | Crohn’s Disease (CD) |
| Disease Distribution | Inflammation begins in the rectum and spreads continuously toward the proximal colon without interruption. | Characterized by patchy involvement with normal areas between inflamed segments, commonly referred to as skip lesions. Rectal involvement may be absent. |
| Pattern of Inflammation | The mucosa typically shows diffuse redness, loss of normal vascular markings, and a granular or friable appearance. | Inflammation is usually focal, asymmetrical, and patchy, producing a characteristic cobblestone appearance. Granularity and friability are less prominent. |
| Ulcer Characteristics | Small superficial ulcers develop within diffusely inflamed mucosa. Severe disease may produce extensive, deep ulcerations. | Multiple aphthous ulcers are common initially and may progress to deep linear or serpiginous ulcers separated by relatively normal mucosa. |
| Appearance of the Colonic Lumen | Chronic disease can result in a narrowed, shortened, and tubular colon. Strictures are uncommon. | Fibrosis and transmural inflammation frequently lead to intestinal narrowing and stricture formation. |
| Rectal Involvement | Rectal involvement is almost always present and often represents the earliest site of disease. | Rectal sparing is relatively common, particularly in isolated ileal disease. |
| Transmural Disease | Inflammation is generally limited to the mucosa and submucosa. | Inflammation extends through the entire bowel wall, increasing the risk of fistulas and abscesses. |
| Typical Endoscopic Hallmark | Continuous colonic inflammation with uniform mucosal involvement. | Patchy inflammation with skip lesions, cobblestoning, and deep longitudinal ulcers. |
Clinical Pearl: Continuous inflammation strongly favors Ulcerative Colitis, whereas skip lesions, cobblestoning, and strictures are classic endoscopic findings suggestive of Crohn’s Disease.
Pathology of Crohn’s disease: Bowel Wall Changes, Skip Lesions, String Sign & Cobblestone Appearance
In Crohn’s disease, chronic inflammation affects the entire thickness of the intestinal wall, leading to significant structural changes. The bowel becomes thickened, rigid, and less flexible. At the same time, the surrounding mesentery often appears swollen, fibrotic, and shortened, which can anchor segments of the intestine in a fixed position.
Because the inflammation is transmural (involving all layers), adjacent loops of bowel may adhere together, forming matted intestinal segments. This process contributes to narrowing of the intestinal lumen and can eventually result in strictures.
A hallmark feature of Crohn’s disease is the presence of “skip lesions”, where inflamed sections of the intestine are interspersed with completely normal areas. In the colon, inflammation that spares the rectum is more suggestive of Crohn’s disease rather than ulcerative colitis.
The earliest visible lesions are aphthous ulcers, which typically develop over lymphoid tissue such as Peyer’s patches in the small intestine or lymphoid aggregates in the colon. As the condition progresses, these small ulcers enlarge and evolve into irregular, star-shaped (stellate) or winding (serpiginous) ulcers.
Over time, these ulcers merge to form deep longitudinal and transverse fissures. The remaining intact mucosa between ulcerated areas creates the classic “cobblestone appearance” seen on endoscopy.

Representative colonoscopic views illustrating common manifestations of Crohn’s disease, including aphthous ulcers, cobblestone inflammatory changes, stellate ulceration, and discontinuous patchy mucosal lesions. These findings help clinicians evaluate disease activity and intestinal involvement.
In advanced disease, fissures may extend deeply through the intestinal wall, reaching the outermost layer (serosa). Additionally, clusters of immune cells (lymphoid aggregates) are often found within and beyond the bowel wall. The presence of non-caseating granulomas is a characteristic histological feature of Crohn’s disease and helps distinguish it from ulcerative colitis.

Radiological features of Crohn’s disease demonstrating multiple strictures and the classic “string sign” in the small intestine on barium follow-through imaging.
- Diet for IBD, Lifestyle Changes & Natural Remedies: What to Eat and Avoid- Click Here
Management of crohn’s disease

Clinical decision tree showing the assessment of Crohn’s disease severity and corresponding treatment strategies, from remission induction to long-term maintenance therapy.
IBD Treatment Explained: Steroids, Biologics, 5-ASA & Immunosuppressants
Treatment of inflammatory bowel disease (IBD) focuses on two main goals: inducing remission (controlling active flare-ups) and maintaining remission (preventing relapse).

Flowchart illustrating evidence-based induction of remission therapies for Crohn’s disease and ulcerative colitis, highlighting biologics, steroids, and advanced treatment options.
Overall, treatment is tailored to the individual, taking into account disease severity, location, response to previous therapies, and risk of complications.
For both ulcerative colitis (UC) and Crohn’s disease (CD), short-term use of corticosteroids (oral or intravenous) is commonly used to manage acute flare-ups. However, long-term use is avoided due to significant side effects, so steroids are typically tapered over 8–12 weeks once remission is achieved.
In ulcerative colitis, aminosalicylates (5-ASA) are first-line treatments for maintaining remission, particularly in mild to moderate disease affecting the distal colon. In more severe cases, or when disease extends further, immunosuppressive therapies may be required. These include:
- Thiopurines (e.g., azathioprine)
- Anti-TNF biologics (e.g., infliximab, adalimumab, certolizumab)
- Janus kinase inhibitors (e.g., tofacitinib)
- Calcineurin inhibitors (e.g., cyclosporine)
For Crohn’s disease, treatment depends on disease severity and location. In mild cases affecting the ileum and proximal colon, budesonide can be used to induce remission and is then gradually discontinued. In moderate to severe disease, more advanced therapies are often needed, including:
- Immunomodulators (thiopurines, methotrexate)
- Biologic therapies (anti-TNF agents, interleukin inhibitors such as ustekinumab)
For patients who do not respond to standard treatments or who become steroid-dependent, integrin receptor antagonists (e.g., vedolizumab) may be used.
STEROIDS Dosing , Safety, Side effects & Monitoring

Comprehensive reference chart outlining steroid medications used in inflammatory bowel disease management, including dosage information, safety considerations, adverse effects, and monitoring recommendations.
Budesonide Class- Steroid
Budesonide MOA (Mechanism of action) and Interactions:
Budesonide is a potent glucocorticoid (corticosteroid) with strong anti-inflammatory properties. It works by binding to intracellular glucocorticoid receptors (GRs), reducing inflammation and suppressing excessive immune responses at both the cellular and genetic levels.
Unlike many medications that act through cell-surface receptors, budesonide enters target cells and activates the glucocorticoid receptor signaling pathway, a type of nuclear receptor pathway. After binding to the glucocorticoid receptor in the cytoplasm, the budesonide-receptor complex moves into the cell nucleus, where it regulates the expression of numerous genes. This process decreases the production of pro-inflammatory cytokines and inflammatory mediators while increasing the synthesis of anti-inflammatory proteins.
One of budesonide’s major advantages is its high local anti-inflammatory activity combined with low systemic exposure. Following oral administration, a significant portion of the drug undergoes extensive first-pass metabolism in the liver, resulting in reduced systemic absorption and a lower risk of corticosteroid-related adverse effects compared with conventional systemic corticosteroids.
Because of its targeted anti-inflammatory action and favorable safety profile, budesonide is widely used in the treatment of inflammatory conditions such as Crohn’s disease, ulcerative colitis, microscopic colitis, asthma, and allergic rhinitis.
Budesonide Drug Interactions:
Budesonide is primarily metabolized by the cytochrome P450 (CYP3A4) enzyme in the liver. Therefore, medications or foods that affect CYP3A4 activity can significantly alter budesonide blood levels, increasing the risk of adverse effects or reducing therapeutic efficacy.
1. CYP3A4 Inhibitors
Strong and moderate CYP3A4 inhibitors can increase budesonide concentrations by slowing its metabolism, leading to a higher risk of systemic corticosteroid side effects such as adrenal suppression, hyperglycemia, and Cushing-like features.
Examples include:
- Ketoconazole
- Itraconazole
- Clarithromycin
- Erythromycin
- Ritonavir and other HIV protease inhibitors
- Cobicistat
- Grapefruit juice and grapefruit products
Recommendation: Avoid concurrent use whenever possible. If combination therapy is necessary, monitor patients closely for corticosteroid-related adverse effects.
2. Immunosuppressive Drugs
Using budesonide with other immunosuppressive medications can further suppress the immune system, increasing the risk of serious bacterial, viral, fungal, and opportunistic infections.
Examples include:
- Azathioprine
- Methotrexate
- Cyclosporine
- Tacrolimus
- Biologic agents (e.g., infliximab, adalimumab)
Recommendation: Use with caution and monitor patients regularly for signs of infection.
3. Antacids
Antacids may increase gastric pH, causing enteric-coated budesonide capsules or tablets to dissolve prematurely. This can reduce drug delivery to the intended site in the intestine and potentially decrease treatment effectiveness.
Recommendation: Administer antacids at least 2 hours before or 2 hours after taking enteric-coated budesonide.
2. Aminosalicylates (5-ASA): Overview and Clinical Uses
Aminosalicylates (5-ASA) are first-line anti-inflammatory medications primarily used to induce and maintain remission in patients with mild to moderate ulcerative colitis (UC). These drugs exert their therapeutic effects locally within the intestinal mucosa, helping reduce inflammation and promote mucosal healing. Although their exact mechanism of action has not been fully established, they are believed to inhibit inflammatory mediators and decrease the production of pro-inflammatory cytokines in the gastrointestinal tract.
Mesalamine (5-ASA)
Mesalamine is the most commonly prescribed aminosalicylate and is considered the preferred 5-ASA agent because of its excellent safety profile and favorable tolerability. It is available in a variety of formulations, including oral tablets, extended-release capsules, rectal suppositories, and enemas, allowing treatment to be tailored according to the location and severity of ulcerative colitis.
Other Aminosalicylates
Other medications in this class include sulfasalazine, balsalazide, and olsalazine. These agents are administered orally and function as prodrugs, meaning they must be metabolized within the colon to release the active compound, mesalamine (5-ASA), which produces the anti-inflammatory effect.
Among these agents, Sulfasalazine Reviews is prescribed less frequently because its sulfapyridine component is associated with a higher incidence of adverse effects, including gastrointestinal intolerance, headache, rash, and hypersensitivity reactions. In contrast, balsalazide and olsalazine generally avoid sulfapyridine-related toxicity while still delivering mesalamine to the colon.
Sulfasalazine rheumatoid arthritis : Sulfasalazine is aslo prescribed in rheumatoid arthritis
Aminosalicylates (5-ASA): Dosing , Safety, Side effects & Monitoring
| Drug | Dosage | Safety, Side Effects & Monitoring |
| Mesalamine Extended-Release (ER) Capsules: Pentasa®, Apriso®, Delzicol® Tablets: Asacol HD®, Lialda® Rectal Enema: Rowasa® Rectal Suppository: Canasa® | Induction TherapyTypically administered for 6–8 weeks (oral formulations) and/or 3–6 weeks (rectal formulations). • Asacol HD: 1.6 g orally three times daily (TID)• Delzicol: 800 mg orally TID • Lialda: 2.4–4.8 g orally once daily • Pentasa: 1 g orally four times daily (QID) • Canasa Suppository: 1 g rectally at bedtime; retain for 1–3 hours • Rowasa Enema: 4 g rectally at bedtime; retain overnight (approximately 8 hours). Maintenance Therapy • Apriso: 1.5 g orally once daily• Delzicol: 1.6 g orally in 2–4 divided doses • Lialda: 2.4 g orally once daily• Pentasa: 1 g orally QID • Rowasa Enema: 2 g rectally at bedtime or 4 g every 2–3 days | Contraindications• Known allergy to salicylates or aminosalicylates. Warnings & Precautions• May cause an acute intolerance syndrome characterized by abdominal cramping, severe abdominal pain, and bloody diarrhea.• Use cautiously in patients with renal or hepatic dysfunction.• Delayed gastric emptying (e.g., pyloric stenosis) may reduce drug delivery to the colon. • Rare hypersensitivity reactions, including myocarditis, pericarditis, nephritis, blood disorders, and multi-organ injury, have been reported.• Older adults (>65 years) may have a greater risk of hematologic abnormalities.• Increased sensitivity to sunlight may occur. • Apriso® contains phenylalanine and should be avoided in phenylketonuria (PKU).• Rowasa® contains potassium metabisulfite, which may trigger allergic reactions in susceptible individuals. Common Side Effects Abdominal discomfort, nausea, headache, gas, belching, and nasopharyngitis. Monitoring• Renal function tests• Liver function tests (LFTs)• Complete blood count (CBC)• Assessment of inflammatory bowel disease (IBD) symptoms. Clinical Notes• Mesalamine generally has better tolerability than other 5-ASA medications. • Rectal mesalamine provides superior benefit for distal ulcerative colitis and ulcerative proctitis compared with oral therapy alone or rectal corticosteroids. • Oral and rectal formulations may be combined for enhanced efficacy. • Asacol HD® and Delzicol® may leave an empty tablet shell (“ghost tablet”) in the stool, which is expected and harmless.• Swallow delayed-release tablets or capsules whole; avoid crushing, chewing, or splitting. • Do not administer Apriso® together with antacids because its release depends on gastric pH. |
| SulfasalazineTablets: Azulfidine® Delayed-Release Tablets: Azulfidine EN-tabs® | Induction TherapyBegin with 3–4 g/day orally in divided doses (TID or QID), then gradually increase to 4–6 g/day as tolerated. Maintenance Therapy2 g/day orally divided into 3–4 doses. | Contraindications• Allergy to sulfonamides or salicylates • Intestinal or urinary tract obstruction• Porphyria. Clinical Notes• Administer doses no more than 8 hours apart to maintain therapeutic drug levels. • If gastrointestinal intolerance develops, dose reduction may improve tolerability. |
| Balsalazide – disodium (Colazal®)Capsules | Induction Therapy2.25 g orally (three 750 mg capsules) three times daily for 8–12 weeks. | Contraindications• Hypersensitivity to salicylates. Warnings & Precautions• Delayed gastric emptying may interfere with drug release in the colon.• Acute intolerance syndrome can occur.• Use with caution in patients with impaired kidney or liver function.• May increase sensitivity to sunlight. Common Side EffectsHeadache, abdominal pain, nausea, vomiting, and diarrhea. Monitoring• Kidney function• Liver function tests• Clinical assessment of IBD activity. Clinical Notes-Capsules may be opened and sprinkled onto applesauce if swallowing is difficult. The granules may be chewed because they are not enteric-coated. Temporary staining of the teeth or tongue may occur. |
| Olsalazine (Dipentum®)Capsules | Maintenance Therapy500 mg orally twice daily (BID).Take with food to reduce gastrointestinal discomfort. | Contraindications• Salicylate hypersensitivity. Common Side EffectsDiarrhea and abdominal pain are the most frequently reported adverse effects. Monitoring• Complete blood count (CBC)• Liver function tests (LFTs)• Renal function tests• Ongoing assessment of inflammatory bowel disease symptoms. |
Thiopurines (Azathioprine & Mercaptopurine) in IBD
Thiopurines, mainly azathioprine and mercaptopurine, are classified as immunosuppressive or immunomodulatory agents. Although they do not have an FDA-approved indication for inflammatory bowel disease (IBD), they are widely recommended in clinical guidelines for both induction and maintenance of remission, often used alone or in combination with other therapies.
Mechanism of Action (MOA) of Thiopurines –

Flowchart illustrating the mechanism of action of thiopurines (azathioprine and mercaptopurine), showing prodrug activation, formation of 6-TGNs, inhibition of purine synthesis, DNA/RNA incorporation, and immunosuppressive effects in inflammatory bowel disease (IBD).
Thiopurine Dosing , Safety, Side effects & Monitoring
| DRUG | DOSING | SAFETY / SIDE EFFECTS / MONITORING |
| Azathioprine (Azasan, Imuran) | Form: Tablet, Injection Dose: 1.5–2.5 mg/kg/day (IV or PO) Renal adjustment: CrCl < 50 mL/min → dose reduction required Administration note: Oral dosing may be taken after meals or in divided doses to reduce GI side effects | BOXED WARNING: • Chronic immunosuppression increases risk of malignancy (especially lymphomas in IBD) • Mutagenic potential • Risk of hematologic toxicity WARNINGS: • Leukopenia, thrombocytopenia, anemia • Higher risk in TPMT deficiency (↑ myelosuppression) • Serious infections • Hepatotoxicity • GI hypersensitivity (N/V/D, rash, fever, ↑ LFTs) SIDE EFFECTS: • Nausea, vomiting, diarrhea • Rash • Elevated liver enzymes (LFTs) MONITORING: • CBC (weekly for first month, then periodically) • LFTs • Renal function • Monitor for malignancy signs NOTES: • Consider TPMT genetic testing before therapy • Azathioprine converts to mercaptopurine → avoid combination use • Aminosalicylates may inhibit TPMT → increased toxicity risk • Allopurinol inhibits metabolism → requires azathioprine dose reduction |
| Mercaptopurine (Purixan) | Form: Tablet, Oral suspension Dose: 1–1.5 mg/kg/day Renal adjustment: CrCl ≤ 50 mL/min → dose reduction required Administration note: Take on empty stomach | SAFETY PROFILE: • Similar toxicity profile to azathioprine • Myelosuppression (leukopenia, thrombocytopenia, anemia) • Increased infection risk • Hepatotoxicity • GI intolerance • Elevated LFTs NOTES: • No boxed warning (unlike azathioprine) • Take on empty stomach for optimal absorption • Avoid term “6-mercaptopurine (6-MP)” → risk of dosing errors (6-fold overdose risk if misinterpreted) |
Immunosuppressants & Biologics in IBD
| Drug/Class | Mechanism of Action | Clinical Use in IBD | Route & Dosing | Key Points / Notes |
| Methotrexate | Folic acid antagonist → inhibits dihydrofolate reductase → ↓ DNA synthesis in rapidly dividing immune cells → anti-inflammatory effect | Induction & maintenance of remission in moderate–severe Crohn’s disease (CD), especially if azathioprine not tolerated | Once weekly IM or SC injection | No FDA approval for IBD but guideline-supported; useful alternative immunomodulator |
| Cyclosporine- | Calcineurin inhibitor → ↓ IL-2 transcription → suppresses T-cell activation | Severe ulcerative colitis (UC), often as rescue therapy | IV continuous infusion or oral | Mainly short-term use; bridge to maintenance therapy |
| Anti-TNF agents (e.g., infliximab Price- A 100-mg vial of infliximab costs £419.62)
| Monoclonal antibodies against TNF-α → block pro-inflammatory cytokine cascade (↓ interleukins, inflammation) | Moderate–severe UC and CD; often used when conventional therapy fails | IV or SC depending on agent | Often combined with thiopurines to reduce antibody formation |
| Ustekinumab (Stelara) ulcerative colitis | Blocks IL-12 & IL-23 → reduces T-cell mediated inflammation | Moderate–severe UC and CD | IV induction → SC maintenance | Can be used even before anti-TNF failure in some patients |
| Risankizumab (Skyrizi) Crohn’s disease | Selective IL-23 inhibitor → blocks Th17 pathway | Moderate–severe Crohn’s disease (CD) | IV induction → SC maintenance | Newer biologic; alternative first/second-line option |
Integrin Receptor Antagonists
Natalizumab and vedolizumab are monoclonal antibodies that target subunits of integrin molecules. By binding to these integrins, they block the interaction between integrins and adhesion molecules, thereby preventing inflammatory cells from migrating into gastrointestinal tissue.
These agents are used for the induction and maintenance of remission in patients with inflammatory bowel disease (IBD), particularly in those who have had an inadequate response to conventional therapies, cannot tolerate standard treatments, or are dependent on steroids.
| Drug | Indications | Dosing | Safety / Side Effects / Monitoring | Key Notes |
| Natalizumab (Tysabri) | Moderate–severe Crohn’s disease in patients who failed or cannot tolerate conventional therapy or are steroid-dependent | 300 mg IV over 1 hour every 4 weeks; discontinue if no response by 12 weeks | Boxed warning: PML (progressive multifocal leukoencephalopathy) → potentially fatal JC virus brain infection; monitor mental status. Risk ↑ with anti-JCV antibodies, prolonged use, prior immunosuppressants. Other: herpes encephalitis/meningitis, hepatotoxicity, hypersensitivity, infections | Available only via REMS TOUCH program; infusion reactions, headache, fatigue, arthralgia, nausea, rash, depression; avoid combination with other immunosuppressants |
| Vedolizumab (Entyvio) | Moderate–severe Crohn’s disease and ulcerative colitis | 300 mg IV at 0, 2, and 6 weeks, then every 8 weeks; discontinue if no benefit by week 14 | Infusion reactions, hypersensitivity, infections, liver injury, rare PML risk | Gut-selective safety advantage; ensure vaccinations up to date; avoid live vaccines during therapy unless necessary |
| Monitoring: LFTs, infection signs, hypersensitivity reactions, neurological symptoms (PML surveillance), TB screening | Refrigeration required; protect from light; reconstitute gently (swirl, do not shake); use immediately or refrigerate ≤4 hours; do not freeze |
Leave a Reply