Inflammatory Bowel Disease (IBD): Types, Symptoms & Pathophysiology
Inflammatory Bowel Disease (IBD):Inflammatory Bowel Disease (IBD) is a group of chronic inflammatory conditions of the gastrointestinal tract caused by abnormal immune system activation.
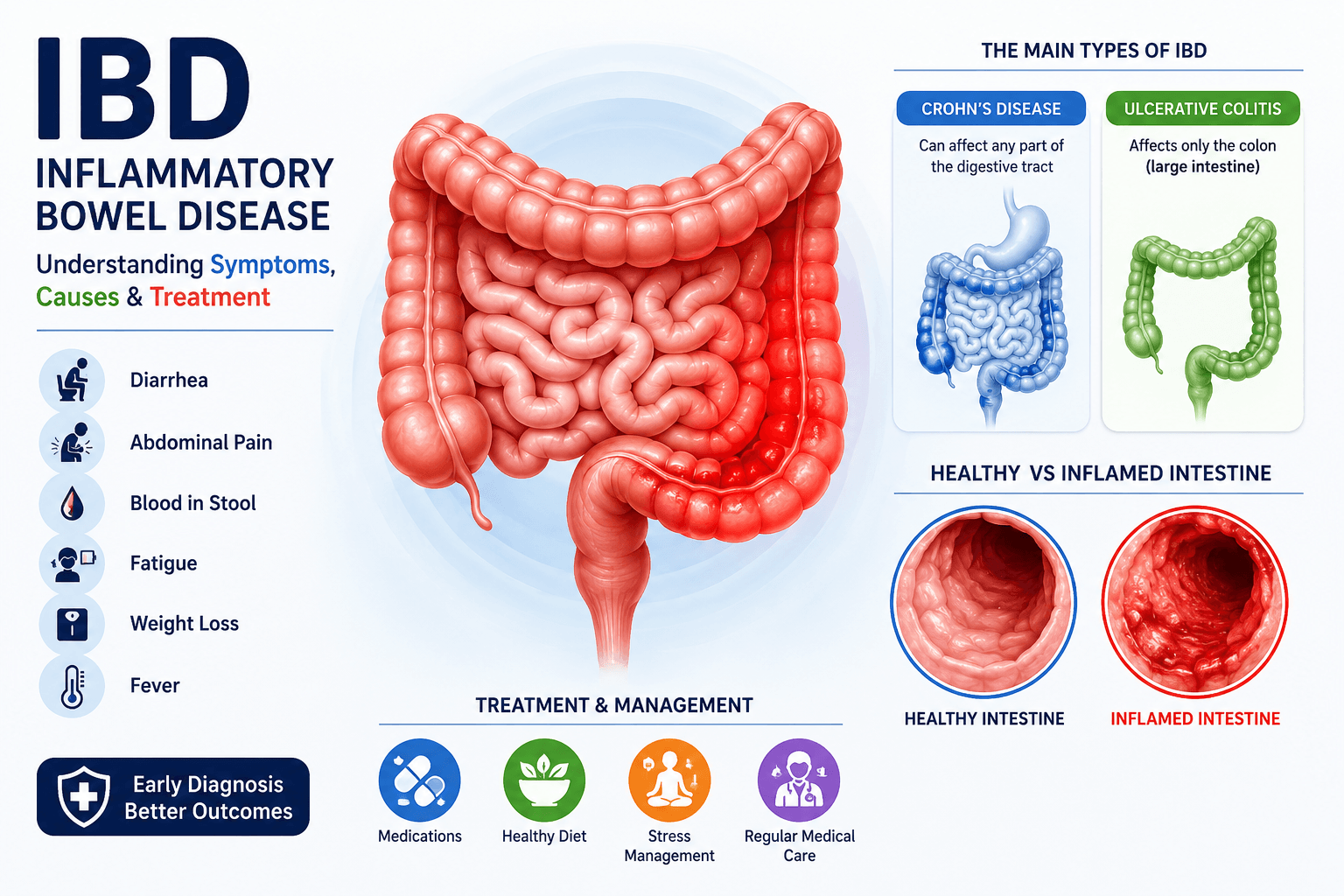
The Types of idiopathic inflammatory bowel diseases include Crohn’s disease, ulcerative colitis, and ulcerative proctitis.
1. Crohn’s disease
Crohn’s disease can affect any part of the gastrointestinal tract, from the mouth to the anus. inflammation occurs in a patchy (discontinuous) pattern, meaning healthy areas of intestine can exist between inflamed segments. The inflammation is also transmural, affecting all layers of the intestinal wall from the mucosa to the serosa and may lead to symptoms such as abdominal pain, diarrhea, and weight loss, along with complications like strictures and fistulas.2. Ulcerative colitis
Ulcerative colitis mainly affects the colon and rectum. It causes continuous inflammation of the inner lining of the colon, leading to symptoms such as bloody diarrhea, abdominal discomfort, and urgency to pass stool.3. Ulcerative proctitis
Ulcerative proctitis is a form of ulcerative colitis that affects only the rectum or less than 30 cm of the distal colon.

Illustration showing the types of Inflammatory Bowel Disease (IBD), including Crohn’s disease and ulcerative colitis, with anatomical distribution and disease patterns in the gastrointestinal tract.
Symptoms of Ulcerative colitis and Symptoms of Crohn’s disease
A common symptom of IBD is bloody diarrhea, along with:
- Rectal urgency
- Tenesmus (feeling of incomplete bowel emptying)
- Abdominal pain and bloating
- Fatigue
- Weight loss (in some cases)
- Nausea and vomiting
- Occasionally constipation
Chronic & Intermittent Nature
IBD is a chronic but relapsing disease, meaning symptoms come and go.
- Flares (exacerbations): periods of active symptoms
- Remission: periods with minimal or no symptoms
Severity can range from mild to severe depending on disease activity.
Common Triggers of Inflammatory Bowel Disease (IBD) Flare-Ups
Flare-ups can occur unpredictably and may be triggered by:
- Infections
- NSAID (painkiller) use
- Certain foods
Common Food Triggers in Inflammatory Bowel Disease (IBD) / diet for inflammatory bowel disease
Triggers vary between individuals but often include:
- Fatty foods
- Gas-producing foods such as lentils, beans, cabbage, broccoli, and onions
Avoiding triggers or modifying food preparation can help reduce symptoms.
Main Diffrence between IBD (Inflammatory Bowel Disease) vs IBS (Irritable Bowel Syndrome)
Irritable Bowel Syndrome can sometimes be confused with IBD because both cause:
- Abdominal pain
- Bloating
- Gas
- Changes in bowel habits (diarrhea or constipation)
However, IBS is not an inflammatory condition and does not cause structural damage to the intestines. In contrast, IBD involves visible inflammation and tissue injury. IBS treatment mainly focuses on symptom relief, while IBD requires anti-inflammatory and immune-modulating therapy.
Pathophysiology of Inflammatory Bowel Disease (IBD)

Scientific illustration of inflammatory bowel disease (IBD) pathology showing intestinal barrier dysfunction, immune cell activation, cytokine signaling, and mechanisms involved in Crohn’s disease and ulcerative colitis.
Pathogenesis of Crohn’s Disease
The development of Crohn’s Disease is complex and involves multiple genetic, immune, and environmental factors. It is not caused by a single defect, but rather by a combination of abnormalities in different body systems.
1. Genetic Factors (Inherited Risk)
Some people have genetic changes that increase their risk of Crohn’s disease.
For example:
- NOD2 gene mutation → weak detection of harmful gut bacteria
- ATG16L1 & IRGM gene variants → defective autophagy (cell’s cleaning and defense system)
These defects reduce the body’s ability to control bacteria in the gut.
2. Weak Innate Immune Response
Normally, the gut has a first-line defense called innate immunity. In Crohn’s disease:
- Paneth cells produce fewer defensins (natural antimicrobial proteins)
- Bacteria are not properly cleared
- This leads to immune overreaction
3. Overactive Adaptive Immune Response
Because of weak early defense, the body activates a stronger immune response:
- Increased Th1 and Th17 cells
- Overproduction of inflammatory signals (especially IL-12 and IL-23 pathways)
This leads to chronic gut inflammation.
4. Role of Inflammatory Cytokines (TNF-α)
Immune cells like macrophages and dendritic cells release TNF-α (Tumor Necrosis Factor-alpha), a key inflammatory molecule that:
- Increases gut inflammation
- Damages intestinal tissue
This is why anti-TNF drugs are effective treatments in Crohn’s disease.
Weak Gut Barrier Function
In Crohn’s disease, the intestinal lining becomes more permeable:
- More bacteria and antigens enter the gut wall
- This triggers continuous immune activation
- Genes like PTGER4 may contribute to this barrier defect
6. Immune Cell Migration (Leukocyte Trafficking)
White blood cells move into the gut through special “adhesion molecules”:
- α4β7 integrin binds MAdCAM-1 (gut-specific pathway)
- α4β1 integrin binds ICAM-1 (widespread inflammation)
This increases immune cell buildup in the intestine and worsens inflammation. Drugs that block this process can reduce disease activity.
Key Summary
Crohn’s disease develops due to:
- Genetic susceptibility
- Weak bacterial sensing
- Overactive immune response
- Barrier dysfunction in the gut
- Excess immune cell migration
Together, these factors cause chronic, relapsing intestinal inflammation.
Early diagnosis and treatment of Inflammatory Bowel Disease are important in both conditions to control inflammation, prevent complications, and improve long-term outcomes.
Difference between crohn’s and ulcerative colitis

Side-by-side infographic comparing ulcerative colitis and Crohn’s disease, highlighting the major differences in pathology, radiologic findings, endoscopic appearance, and overall disease distribution to aid diagnosis and medical learning.
Diet for crohn’s disease and ulcerative colitis
Managing inflammatory bowel disease (IBD) involves important lifestyle and dietary adjustments to reduce symptom flare-ups and improve gut health. Patients are generally advised to identify and avoid trigger foods that worsen symptoms.
Eating smaller, more frequent meals that are low in fat and dairy may help reduce digestive discomfort. Adequate hydration is essential, so increasing water intake is strongly recommended. Foods high in fibre can be gradually introduced depending on individual tolerance.
Certain substances should be limited or avoided, including alcohol, caffeine, and carbonated drinks, as they can irritate the gastrointestinal (GI) tract and worsen symptoms such as bloating and diarrhoea. Additionally, ingredients like sorbitol (a common artificial sweetener) and lactose may trigger symptoms, particularly in individuals with lactose intolerance.
For symptom relief, some patients may use medications such as antidiarrhoeals or antispasmodics (e.g., dicyclomine) under medical supervision. However, these are not suitable for everyone and should be used cautiously, especially in severe disease or after bowel surgery. Opioid medications are generally avoided due to the risk of constipation and serious complications like toxic megacolon.
Nutritional deficiencies are common in IBD, so vitamin and mineral supplementation (including vitamin B12, folate, vitamin D, calcium, iron, and zinc) may be necessary to support overall health.
The effects of nicotine differ depending on the type of IBD—it may worsen Crohn’s disease but sometimes shows limited benefit in ulcerative colitis. However, due to potential side effects, its use is not routinely recommended.
Some patients benefit from probiotics, particularly strains such as Lactobacillus and Bifidobacterium infantis, which may help reduce symptoms like bloating, abdominal pain, and irregular bowel habits. Additionally, omega-3 fatty acids (found in fish oils) may have mild anti-inflammatory effects, although evidence remains limited.
Natural remedies such as peppermint, chamomile, horehound, and wheatgrass are sometimes used as supportive therapies, but their effectiveness varies between individuals.
Leave a Reply